Monday, 10 November 2008
Medication for Obesity
Prescription weight-loss medication
It's best to lose weight through a healthy diet and regular exercise. But if you're among those who struggle to lose weight and the excess weight has produced medical problems, prescription weight-loss drugs may be able to help you.
Your doctor may consider you a candidate for medication treatment if these criteria apply:
- Other methods of weight loss haven't worked for you.
- Your body mass index (BMI) is greater than 27 and you have medical complications of obesity, such as diabetes, high blood pressure or sleep apnea.
- Your BMI is greater than 30.
Two prescription drugs have been approved by the Food and Drug Administration (FDA) for long-term weight loss. These drugs work in different ways and cause different side effects.
- Sibutramine (Meridia). This drug changes your brain chemistry, making you feel full
 more quickly. Though sibutramine generally helps you lose more weight than you could through diet and exercise alone, it's no magic bullet. Studies have shown that after a year, sibutramine users lost an average of about 10 pounds more than did people simply following a low-calorie diet and taking a placebo. Side effects can include increased blood pressure, headache, dry mouth, constipation and insomnia.
more quickly. Though sibutramine generally helps you lose more weight than you could through diet and exercise alone, it's no magic bullet. Studies have shown that after a year, sibutramine users lost an average of about 10 pounds more than did people simply following a low-calorie diet and taking a placebo. Side effects can include increased blood pressure, headache, dry mouth, constipation and insomnia. - Orlistat (Xenical). This drug prevents the absorption of fat in your intestines.
 Unabsorbed fat is eliminated in the stool. Average weight loss with orlistat is modest — about 6 pounds after one year. Side effects associated with the drug include oily and frequent bowel movements. Because orlistat blocks absorption of some nutrients, your doctor will recommend that you also take a multivitamin. The FDA has approved a reduced-strength version of orlistat (Alli) to be sold without a prescription. This medication works the same as prescription-strength orlistat and is meant only to supplement — not replace — a healthy diet and regular exercise.
Unabsorbed fat is eliminated in the stool. Average weight loss with orlistat is modest — about 6 pounds after one year. Side effects associated with the drug include oily and frequent bowel movements. Because orlistat blocks absorption of some nutrients, your doctor will recommend that you also take a multivitamin. The FDA has approved a reduced-strength version of orlistat (Alli) to be sold without a prescription. This medication works the same as prescription-strength orlistat and is meant only to supplement — not replace — a healthy diet and regular exercise.


Surgical Treatment of Obesity
Obesity is a chronic medical condition without a "cure." For severely obese patients who have significant obesity-related medical complications (hypertension, diabetes, sleep apnea, etc.), surgery is an option. Generally, the weight criterion for surgery is to be at least 100 lbs. (45 kg.) over your ideal body weight. The surgical methods have changed over the years but can be divided into gastric (stomach) restrictive procedures and gastrointestinal (intestinal) bypass procedures.
Gastric (stomach) restrictive procedures
Vertical Banded Gastroplasty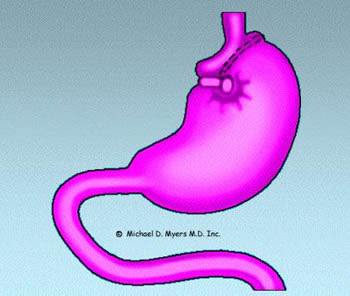
The gastric restrictive procedures are performed in many medical centers. One of the most widely used procedures is the vertical banded gastroplasty (VBG) sometimes with additional reinforcement of a small silastic ring. In VBG, the stomach is "stapled" to reduce its capacity to approximately 15 ml. (1/2 oz.) and a silastic ring is inserted to help prevent the stomach from "stretching" in size. What is formed is essentially a small stomach "pouch" that receives food from the esophagus and a much larger, unstapled stomach that receives small amounts of food from the proximal "pouch". When one eats, only a small amount of food can be consumed without the pouch becoming distended. This generally leads to a feeling of satiety or fullness. If one continues to eat, one will develop nausea, vomiting, or pain, which generally results in the termination of eating. Patients must adapt to their new, restricted stomach size and restrict their food intake to prevent these side-effects. Complications can result from the surgery. When gastroplasty is done by well-trained physicians, the mortality (death rate) from the surgery is under 1 %. 
Complications include risk of infection, obstruction (blockage) of the outlet necessitating surgical revision, development of blood clots in the legs or lungs, bleeding, metabolic or nutritional deficiencies (including protein calorie malnutrition), and recurrent vomiting. It is not uncommon to slowly develop vitamin (especially vitamin B-12) and mineral deficiencies resulting in anemia or osteoporosis (softening of the bones). After the surgery, the patient must be followed by physicians who are familiar with the long-term complications and required long-term treatment.
The effectiveness of the surgery is fair with average weight loss being between 50 and 100 lbs. (or about a loss of about 25% of initial weight) with about 50% of the weight loss being maintained at 5 years. It is generally common for the body weight to slowly increase after the first or second year. The surgery requires a modified diet to prevent nausea and vomiting and to help prevent other long-term side effects. Additionally, one can (partially) bypass the "restriction" by eating calorie-dense liquids such as ice cream or regular soda. Long-term changes in eating habits must take place in order for the surgery to be successful. Vertical Banded Gastroplasty, however, is a viable treatment alternative for severely overweight individuals but again, it is not a cure.
Gastric Banding |

The European literature (where the procedure has been performed for the last few years) show that weight loss is similar to the weight loss seen with vertical banded gastroplasty. The European literature thus far shows a relatively low incidence of side effects and surgical complication.
A major concern with this surgery is that it is, in essence, an old surgery (gastric banding) that was abandoned in the 1980's because of a high incidence of complications (bleeding and obstruction). Although this new approach is less invasive than the "old" banding procedure and the band is adjustable, this procedure is in essence a take-off on a bad basic procedure (gastric banding) which will likely result in the same long-term complications that occurred with the "old" surgery.
Gastrointestinal bypass procedures |

There is usually only mild malabsorption of nutrients (as compared to the old intestinal bypass surgery). Individuals undergoing this surgery will lose significant amounts of weight (mainly fat as opposed to lean body mass or muscle tissue) with about 50-60% of excess body weight being lost initially. Weight maintenance is generally excellent with usually only small increases in weight occurring over 5 years. Like any obesity surgery, the patient will require lifelong medical follow-up and treatment of the medical complications that usually occur (e.g., vitamin B12 deficiency and anemia).
This procedure can now be done laparoscopically, which offers a faster surgical recovery but with the potential of more severe surgical complications since it is a technically difficult procedure. The availability of new state of the art 3-D visualization equipment may make the laparoscopic Roux-en-Y Gastric Bypass the procedure of choice for individuals electing to undergo surgical intervention for their obesity.
For a QuickTime movie (208 KB /approximately 60 seconds download with 28.8 modem) illustrating a a roux-en-y bypass, please click here (animation compliments of Vista Medical Technologies). If you don't have QuickTime, you may download it from Apple Computer (it works great on Macs and PC's) by clicking here.
Biliopancreatic bypass procedures (and similar extensive intestinal bypass procedures)
In these procedures, the digestive juices from the liver and pancreas are diverted to the distal small intestine near the entrance to the large intestine. Thus, food enters the stomach, rapidly transverses the distal small intestine (where absorption of nutrients primarily occurs), and is then delivered to the large intestine (where excess water from the stool is removed). This results in marked malabsorption of nutrients with subsequent marked weight loss (up to 80% of excess body weight). Since there is marked malabsorption of essential nutrients, the probability of vitamin, mineral, and protein-calorie malnutrition is significant. These procedures are probably best avoided at this time since the marked nutrient malabsorption may result in very severe long-term complications that may be similar to the old intestinal bypass operation.
source : http://www.weight.com/obesitysurgery.html